
COVID-19: how does it work? Three propagation circles and the concept of critical mass effect.
I have been looking for a concept that would allow us to better understand how SARS-CoV-2 acts and to explain it simply. This may be of course a little bit simplistic. This framework can be improved but seems helpful to me and can help me understand some blur areas. This is the result of three months of observation. It is based on some scientific data, but also partially on elements not yet demonstrated (such as the concept of critical mass). For the latter, I foresee no other explanation in the immediate future. This epidemic is unusual. We are observing some features shared with other epidemics. On the other hand, some others are different, such as the absence of any pre-existing immunization.
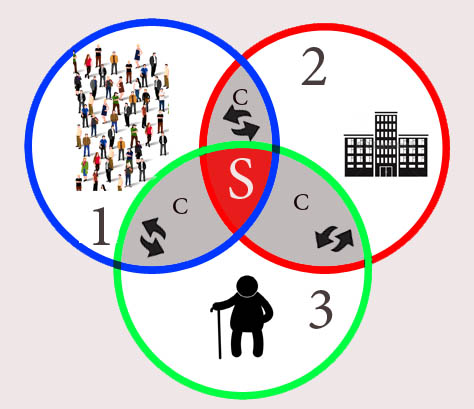
We have three propagation circles.
It is useful to divide the whole population into three different groups: the dynamics of the epidemic are different from one group to the others (e.g. because of mean age, application of prevention measures...)
At the intersection of these 3 circles, we have symptomatic people (S Area) . They account for a small minority. To date, the total number of people who had COVID can be estimated at 7 million in France. PCR Tests have allowed to identify less than 3% (170,000) of them. The case-fatalty rate is estimated to be around 0,5% according to data from the CDC.
- Circle #1: asymptomatic transmission
This circle is composed of the young population in good health. They have many social interactions and travel a lot. They are mostly vectors of the disease. Asymptomatic transmission occurs in this circle at the beginning of the epidemic, before the exponential rise in cases. Symptomatic and severe cases are seldom. SARS-CoV-2 continues to spread in this circle after the initial exponential growth.
- Circle #2: critical mass events
This circle includes gatherings in enclosed places (workplaces, hospitals, continuing care facilities, coffee shops, restaurants, gyms, cinema...). Infected people coming from circle #1 participate in such events, thus disseminating the infection. As the number of infected individuals increases, the viral load increases in the air, until it reaches a critical aerosol load threshold. These events are major driving forces in the dynamics of the epidemic. Superspreaders, rather harmless outdoors, will also massively contaminate these places.
- Circle #3: people at risk and elderly
Elderly and people at risk are the less mobile folks. Being rather immobile, they are undergoing vectorization rather than participating in the dissemination of the disease. This circle comprises those who are the most severely impacted by COVID-19, especially in the early stages of the epidemic. The fatality rate is higher in this group. These 3 circles overlap one with each other. E.g., circle #3 (elderly) overlaps with circle #2 (enclosed places) if we have in mind residents of long care facilities.
Overlapping areas are called "corridors" (C): they illustrate flows between the 3 groups and provide insight for preventive measures.
How does this concept work? Circle #2 has raised much attention. Clusters are located in this circle (e.g. in hospitals or in long term care facilities). The corridor between this circle and the group of people at risk (circle #3) constitutes a major risk factor. E.g., infected people may be discharged from the hospital to nursing homes. Public transportation also plays a major role in the dissemination of COVID-19.
The absence of masks in enclosed places (work, transportation) have made them places of vectorization of this epidemic. This is subsequently affecting people at risk (circle 3). Besides, with increased aerosol loads and repeated exposures, young people with no risk factors may develop COVID-19, especially during the peak of the epidemic.
Circle #2 is also porous towards circle #1: This illustrates how the epidemic spreads from one enclosed place to another.
During lockdowns, circle #1 was most impacted, with delayed effects on the number of symptomatic people. Physical distancing and travel restrictions have impacted this circle, with subsequent and delayed effects on circles #2 and #3.
Circle #2 was impacted by lockdowns, probably more because of better prevention in hospitals (although subjected to shortages in the supply chain), massive staff testings. In the meantime, insufficient contact tracing in the industries has contributed to the vectorization of the disease.
The lifting of travel restrictions is currently accompanied by a low-level increase in the transmission in circle #1. It is very likely that at the same time, not much is happening in both circles #2 and #3. Events in circle #2 will probably be driven by the increase of superspreaders or multiple asymptomatic shedders in one place.
Controlling the propagation in circle #1 is not easy. We can tackle clusters (circle #2). How can we stop the circulation of SARS-CoV-2 in circle #1? Controlling the transmission would help, as well as immunity (humoral, cellular, and local with IgA). These are hypotheses. Extinguishing the circulation of the virus in circle #1 is the aim of some Asian countries, which makes sense. The main vector is young people. They are rarely impacted by the disease, but they play a large role in its spread to other people at higher risk.
thanks for the english version corrections : Quentin Durand Moreau MD Inscrivez-vous au blog
Soyez prévenu par email des prochaines mises à jour
Rejoignez les 232 autres membres